Analysis of Graft Survival in Pediatric Patients Undergoing Kidney Transplantation
Keywords:
Pediatrics, Kidney Transplant, Chronic Renal Failure, Survival AnalysisAbstract
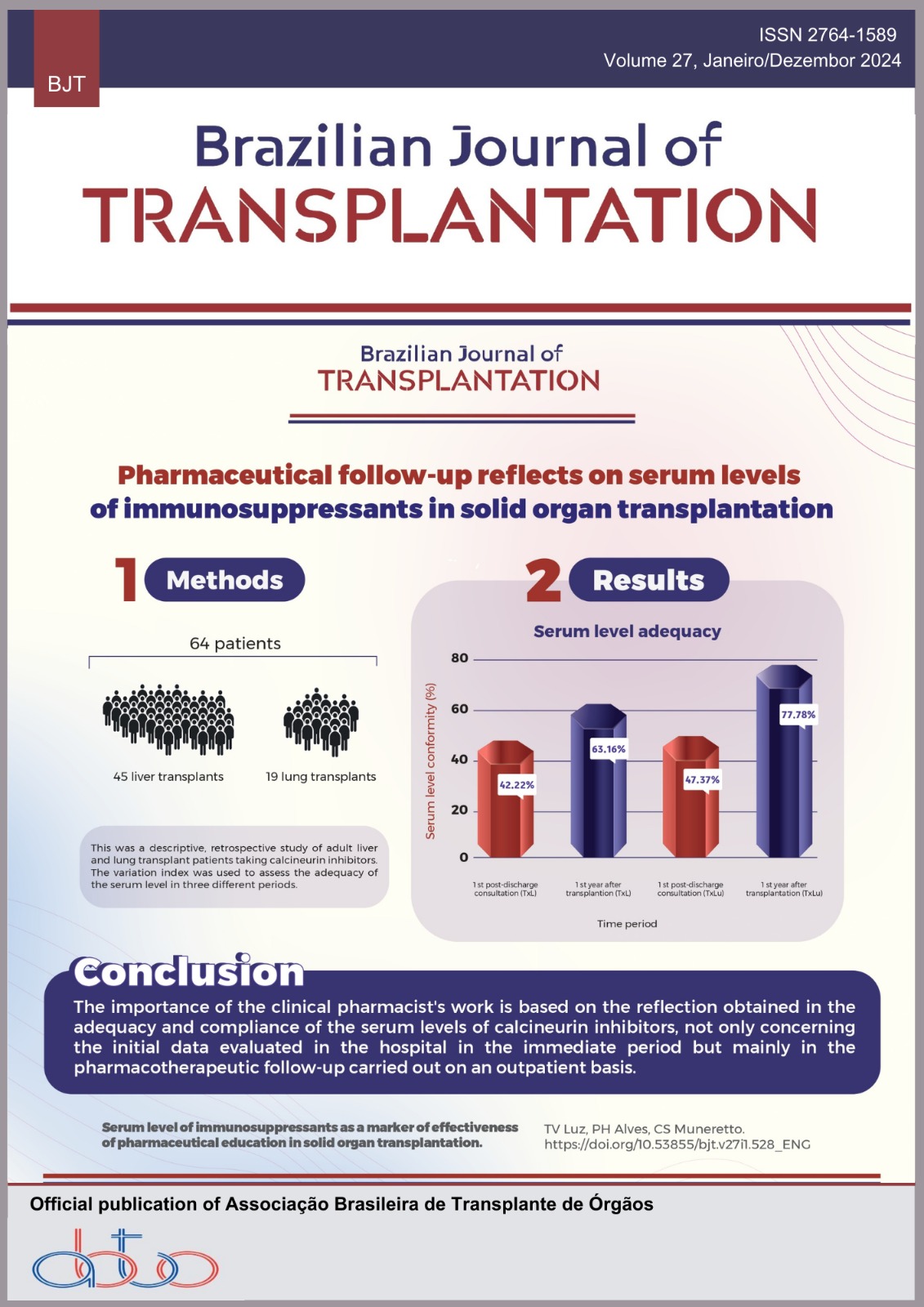
Introduction: Kidney transplantation is the gold standard therapy for end-stage chronic kidney disease (CKD). However, aspects related to the characteristics of the donor and the recipient, the surgical technique, the immunosuppression protocol and comorbidities can impact graft survival. Objectives: To evaluate factors associated with graft survival in pediatric patients undergoing kidney transplantation. Methods: Descriptive, retrospective cohort study, which included all patients aged 1 to 18 years who underwent kidney transplantation at Unidade Renal Pediátrica of Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), Recife, Brazil, from January 2017 to December 2021, with a minimum follow-up time of 10 months, totaling 51 patients. The IMIP ethics and research committee approved the study under CAAE: 52023921.1.0000.5201. Results: The median age of patients undergoing kidney transplantation was 12 years (9-13); 27 (52.9%) were male and eight (15.6%) were younger than 5 years of age. The main etiologies of CKD were congenital anomalies of the kidney and urinary tract (n = 25; 49%). As for kidney transplants, 49 (96.1%) were from a deceased donor and the median follow-up time was 32 (14-42) months. After transplantation, 58% of the population were hypertensive, while 80.4% had dyslipidemia. The 5-year graft and patient survival rates, assessed using the Kaplan Meier curve, were 86.3 and 90.2%, respectively. Seven (n = 5) patients lost the graft, the most common cause being renal vein thrombosis. Nonglomerular causes of CKD showed lower graft survival when compared to glomerular causes (log rank p = 0.035). Conclusion: Our sample’s graft and patient survival rates are similar to national and global data. The most frequent causes of graft loss were thromboembolic events. Furthermore, we observed a high prevalence of hypertension and dyslipidemia. These results direct us to establish strategies to improve survival in pediatric kidney transplants.
Downloads
References
Verghese PS. Pediatric kidney transplantation: a historical review. Pediatr Res 2017;81(1-2):259-64. https://doi.org/10.1038/pr.2016.207
Etesami K, Lestz R, Hogen R. Pediatric kidney transplantation in the United States. Curr Opin Organ Transplant 2020;25(4):343-7. https://doi.org/10.1097/MOT.0000000000000783
Keith DS, Vranic G, Barcia J, Norwood V, Nishio-Lucar A. Longitudinal analysis of living donor kidney transplant rates in pediatric candidates in the United States. Pediatr Transplant 2017;21(2):e12859. https://doi.org/10.1111/petr.12859
North American Pediatric Renal Trials and Collaborative Studies. NAPRTCS 2014 Annual Transplant Report [access on 20 Feb 2024]. Available at: https://naprtcs.org/system/files/2014_Annual_Transplant_Report.pdf
Larkins NG, Wong G, Alexander SI, McDonald S, Prestidge C, Francis A, et al. Survival and transplant outcomes among young children requiring kidney replacement therapy. Pediatr Nephrol 2021;36(8):2443-52. https://doi.org/10.1007/s00467-021-04945-9
Souza VC, Garcia CD, Pestana JM, Stopa Martins SB, Custódio LFP, Bittencourt V, et al. Collaborative Brazilian pediatric renal transplant registry (CoBrazPed-RTx): a report from 2004 to 2018. Pediatr Transplant 2019;23(6):e13463. https://doi.org/10.1111/petr.13463
Torricelli FCM, Watanabe A, David-Neto E, Nahas WC. Current management issues of immediate postoperative care in pediatric kidney transplantation. Clinics (São Paulo) 2014;69(Suppl 1):39-41. https://doi.org/10.6061/clinics/2014(sup01)07
Prudhomme T, Mesnard B, Abbo O, Banuelos B, Territo A. Postoperative surgical complications after pediatric kidney transplantation in low weight recipients (<15 kg): a systematic review. Curr Opin Organ Transplant 2023;28(4):297-308.https://doi.org/10.1097/MOT.0000000000001074
Keller AK, Jorgensen TM, Jespersen B. Identification of risk factors for vascular thrombosis may reduce early renal graft loss: a review of recent literature. J Transplant 2012. https://doi.org/10.1155/2012/793461
Beatrice JM, Takahashi MS, Celeste DM, Watanabe A, Koch VHK, Carneiro JDA. Thromboprophylaxis after kidney transplantation in children: ten-year experience of a single Brazilian center. Pediatr Transplant 2021;25(8):e14101. https://doi.org/10.1111/petr.14101
Bapistella S, Zirngibl M, Buder K, Toulany N, Laube GF, Weitz M. Prophylactic antithrombotic management in adult and pediatric kidney transplantation: a systematic review and meta-analysis. Pediatr Transplant 2021;25(4):e14021. https://doi.org/10.1111/petr.14021
Gander R, Asensio M, Royo GF, Molino JA, García L, Madrid A, et al. Vascular thrombosis in pediatric kidney transplantation: graft survival is possible with adequate management. J Pediatr Urol 2018;14(3):222-30. https://doi.org/10.1016/j.jpurol.2018.01.027
Avilez ND, Souza ABP, Domenico BRD, Prates LC, Mazzali M, Lima ML. Analysis of factors related to the success of pediatric kidney transplantation: a 35 years experience. Transplant Proc 2024;56(1):44-9. https://doi.org/10.1016/j.transproceed.2023.11.002
Al Midani A, Rudarakanchana N, Nagra A, Fidan K, Tugtepe H, Matthias M, et al. Low-dose aspirin reduces the rate of renal allograft thrombosis in pediatric renal transplant recipients. Exp Clin Transplant 2020;18(2):15763. https://doi.org/10.6002/ect.2018.0358
Buder K, Zirngibl M, Bapistella S, Nadalin S, Tönshoff B, Weitz M. Current practice of antithrombotic prophylaxis in pediatric kidney transplantation – Results of an international survey on behalf of the European Society for Paediatric Nephrology. Pediatr Transplant 2020;24(7):e13799. https://doi.org/10.1111/petr.13799
Moudgil A, Martz K, Stablein DM, Puliyanda DP. Good outcome of kidney transplants in recipients of young donors: a NAPRTCS data analysis. Pediatr Transplant 2011;15(2):167-71. https://doi.org/10.1111/j.1399-3046.2010.01432.x
Dale-Shall AW, Smith JM, McBride MA, Hingorani SR, McDonald RA. The relationship of donor source and age on short- and long-term allograft survival in pediatric renal transplantation. Pediatr Transplant 2009;13(6):711-8. https://doi.org/10.1111/j.1399-3046.2008.01054.x
Lima MGDR. Curso clínico de uma coorte de pacientes pediátricos submetidos ao transplante renal: uma análise de sobrevida. Thesis [Master in Science Healthy] – Universidade Federal de Minas Gerais; 2012.
Winterberg PD, Garro R. Long-term outcomes of kidney transplantation in children. Pediatr Clin North Am 2019;66(1):269-80. https://doi.org/10.1016/j.pcl.2018.09.008
Mosca S, Gregório B, Costa T, Correia-Costa L, Mota C. Pediatric kidney transplant and cardiometabolic risk: a cohort study. J Bras Nefrol 2022;44(4):511-21. https://doi.org/10.1590/2175-8239-JBN-2021-0202
Ashoor IF, Dharnidharka VR. Non-immunologic allograft loss in pediatric kidney transplant recipients. Pediatr Nephrol 2019;34(2):211-22. https://doi.org/10.1007/s00467-018-3908-4
Mousavi SSB, Valavi E, Aminzadeh M, Shahbazian H, Otukesh H, Hoseini R, et al. Changes in body mass index after pediatric renal transplantation. Saudi J Kidney Dis Transpl 2020;31(2):448-53. https://doi.org/10.4103/1319-2442.284020
Mitsnefes MM, Khoury PR, McEnery PT. Early posttransplantation hypertension and poor long-term renal allograft survival in pediatric patients. J Pediatr 2003;143(1):98-103. https://doi.org/10.1016/S0022-3476(03)00209-9
Ponticelli C, Citterio F. Non-immunologic causes of late death-censored kidney graft failure: a personalized approach. J Pers Med 2022;12(8):1271. https://doi.org/10.3390/jpm12081271
Bock ME, Wall L, Dobrec C, Chandran M, Goebel J. Management of dyslipidemia in pediatric renal transplant recipients. Pediatr Nephrol 2021;36(1):51-63. https://doi.org/10.1007/s00467-019-04428-y
Habbig S, Volland R, Krupka K, Querfeld U, Strologo LD, Noyan A, et al. Dyslipidemia after pediatric renal transplantation – The impact of immunosuppressive regimens. Pediatr Transplant 2017;21(3):e12914. https://doi.org/10.1111/petr.12914
Francis A, Johnson DW, Melk A, Foster BJ, Blazek K, Craig JC, et al. Survival after kidney transplantation during childhood and adolescence. Clin J Am Soc Nephro. 2020;15(3):392-400. https://doi.org/10.2215/CJN.07070619
Amaral S. Secular trends in survival outcomes of kidney transplantation for children: is the future bright enough? Clin J Am Soc Nephrol 2020;15(3):308-10. https://doi.org/10.2215/CJN.00370120
Dierickx D, Habermann TM. Post-transplantation lymphoproliferative disorders in adults. N Engl J Med 2018;378(6):549-62. https://doi.org/10.1056/NEJMra1702693
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2024 Ligia Soeiro, Anna Clara de Moura Lima, Alice Pimentel Vinicius Silva, Maria Eduarda Cardoso de Araújo, Daniela Saraiva Guerra Lopes, Iracy de Oliveira Araújo, Emília Maria Danta Soeiro

This work is licensed under a Creative Commons Attribution 4.0 International License.